

IN-OFFICE DIAGNOSTIC NEEDLE ARTHROSCOPY USING THE NANOSCOPE ARTHROSCOPY SYSTEM
Diagnostic needle arthroscopy performed in office is a safe and cost-effective method for accurate evaluation of intra-articular pathology, improving clinical decision making. This minimally invasive approach is an effective alternative to traditional diagnostic techniques of diagnostic surgical arthroscopy and magnetic resonance imaging (MRI). Needle arthroscopy is considered low-risk, with an extremely low complication rate when performed with appropriate technique and indications. The purpose of this article is to describe an approach to an in-office diagnostic procedure using a needle arthroscopy system.
Preprocedure Evaluation and Processes
A thorough evaluation is performed on the patient, including medical history and physical examination. The patient undergoes standard weight-bearing radiographs of the knee, including anterior-posterior, lateral, merchant, and posterior-anterior flexion (Rosenberg) views, as well as bilateral long-leg weight-bearing alignment radiographs when indicated. MRI may be performed in addition to the needle arthroscopy when pathology of the bone (i.e., bone marrow edema-like reactions and/or bone involvement in osteochondral defects) and/or extra-articular anatomy, requires evaluation. Risks, benefits, and alternatives to the procedure are discussed with the patient, informed consent is obtained, and a procedural time-out is performed.
Procedural Steps
The patient is positioned supine on the examination table, and can either lie down on the table or sit up leaning against the back of the table or wall if they wish to observe the procedure. The NanoScope™ (Arthrex Inc.) console is placed in proximity to the patient area and facing the surgeon outside of the sterile field. The affected knee is preliminarily prepped with alcohol and chlorhexidine. The desired portal site (standard anterolateral or anteromedial portal) is identified, and a 25-gauge needle is used to inject approximately 7.5 cc of a mixture of local anesthetic, including 1% lidocaine with epinephrine and 0.5% Marcaine without epinephrine at the capsule only, creating a wheel (Fig 1).

Figure 1 - Clinical photograph demonstrating the authors’ preferred approach to in-office needle arthroscopy (left knee). Standard anterolateral and anteromedial portals are shown. With the patient seated and the knee flexed to approximately 90 degrees, a 25-gauge needle is used to inject local anesthetic at one or both portal sites, staying superficial at the skin, making a wheel.
The epinephrine is helpful to improve hemostasis at the portal site(s). Both portal sites can be anesthetized if the surgeon anticipates using both portals during the procedure (i.e., one for viewing and one for probing), although for diagnostic purposes alone, the authors prefer to only anesthetize a single. Next, a sterile field adjacent to the examination table with either a mayo stand or side table is prepared with sterile, disposable drapes. The NanoScope™ (Arthrex Inc.) handpiece kit is opened and placed onto this field in preparation for the procedure. The skin over the anterior aspect of the knee, from the superior pole of the patella to the region of the distal patellar tendon prepped with chlorhexidine, and drapes are placed along the superior and inferior borders of this sterile field, creating a working space centered over the patella. Next, using an 18- or 20-gauge needle, ∼20 cc of 0.25% Marcaine without epinephrine is injected into the joint (Fig 2, Fig 3).

Figure 2 - Clinical photograph (left knee) demonstrating the lateral side of the knee prior to introducing the needle-scope. After the local anesthetic has been injected superficially, the knee is re-prepped with chlorohexidine, after which, sterile drapes are placed.

Figure 3 - Clinical photograph (left knee) demonstrating the use of sterile drapes proximally (along the distal femur) and distally (along the proximal tibia), creating a sterile field prior to introduction of the needle scope.
After a few minutes, the 2.2-mm inflow NanoScope™ (Arthrex Inc.) sheath with sharp trocar is inserted through the anterolateral (or anteromedial) portal into the knee joint, the trocar is withdrawn, the one way stop valve is attached, and the 1.9-mm NanoScope™ (Arthrex Inc.) is inserted (Fig 4).
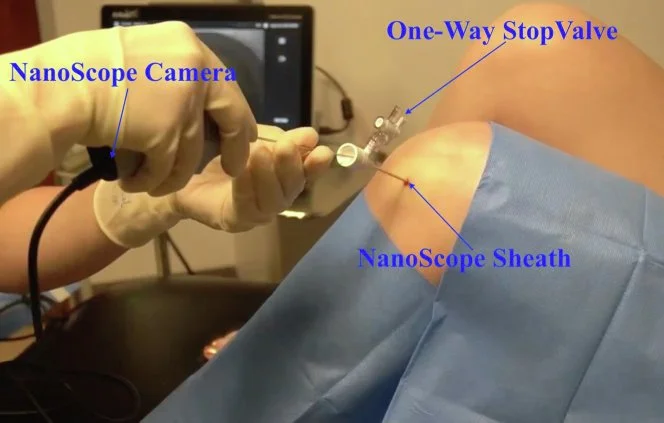
Figure 4 - Clinical photograph (left knee) demonstrating introduction of the 2.2mm inflow NanoScope (Arthrex Inc.) sheath with sharp trocar through the anterolateral portal into the joint. After successful insertion into the joint, the trocar is removed, and the one-way stop valve is attached to the sheath. Next, the 1.9-mm NanoScope (Arthrex Inc.) is inserted through the sheath. A 30-cc syringe of sterile 0.9% normal saline is then connected to the one-way stop valve, and the saline is used to insufflate the joint.
A 30-cc syringe of sterile 0.9% normal saline is then connected to the NanoScope™ (Arthrex Inc.) via the one-way stop valve, the valve is opened, and the saline is used to insufflate the knee. This is followed by the injection of additional saline, up to 90-100 mL total, injected as needed to insufflate the joint and improve visualization. The diagnostic arthroscopy of the knee is then performed on the basis of the patient’s clinical history, physical examination, and any previously obtained diagnostic imaging (Fig 5, A and B)

Figure 5 - (A) View of the lateral side of the left knee. Inset is an arthroscopic view of the left knee through the anterolateral portal site. After insufflating the joint with 30 cc of sterile 0.9% normal saline, additional sterile saline can be injected via the one-way stop valve as needed during the diagnostic procedure to improve visualization. A standard diagnostic arthroscopy of the left knee is performed, as pictured in the inset. (B) View of the lateral side of the left knee. Inset is an arthroscopic view of the left knee through the anterolateral portal site. The medial femoral condyle full-thickness osteochondral defect is identified (pictured in the inset).
Using the opposite portal, a NanoProbe™ (Arthrex Inc.) may be used to evaluate the pathology, particularly useful for sizing chondral defects and/or probing the meniscus (Fig 6).

Figure 6 - Clinical photograph (left knee). Inset is an arthroscopic view of the left knee through the anterolateral portal site. The medial femoral condyle defect is being probed with a NanoProbe (Arthrex Inc.) through the anteromedial portal, which is the accessory portal, as pictured in the inset. This provides the ability to assess the pathology in question and further evaluate the entirety of the joint.
If necessary, the scope may be alternated between the anterolateral and anteromedial portal sites, depending on required visualization, although the authors preference is to maintain efficiency of the procedure by avoiding unnecessary withdrawal and subsequent reintroduction of the scope. At the conclusion of the procedure, all previously insufflated saline is aspirated via the stop valve, and the NanoScope™ (Arthrex Inc.) is removed (Fig 7). A sterile dressing with Steri-Strips, 4×4" gauzes, and an ace-wrap is then applied. The post-procedural plan includes permitted weight-bearing and range of motion, as tolerated, and the use of acetaminophen and/or NSAIDs for pain control. No narcotics are prescribed post-procedure, and no sedatives are used before or during the procedure.

Figure 7 - Clinical photograph (left knee), demonstrating the authors' preferred technique of aspirating as much fluid as possible through the scope at the conclusion of the procedure. The scope is removed and the portal sites are dressed with Steri-Strips, gauze, and an ACE wrap. The patient is allowed immediate weight-bearing as tolerated and range-of-motion as tolerated.
Click on the link for the full print article and video:
In-Office Diagnostic Needle Arthroscopy Using the NanoScope™ Arthroscopy System - PMC (nih.gov)
Published November 2022 in Arthroscopy Techniques (Volume 11 - Issue 11).